Which treatment option should you choose for colon cancer?
2023/11/02
Report
ADVERTISEMENT
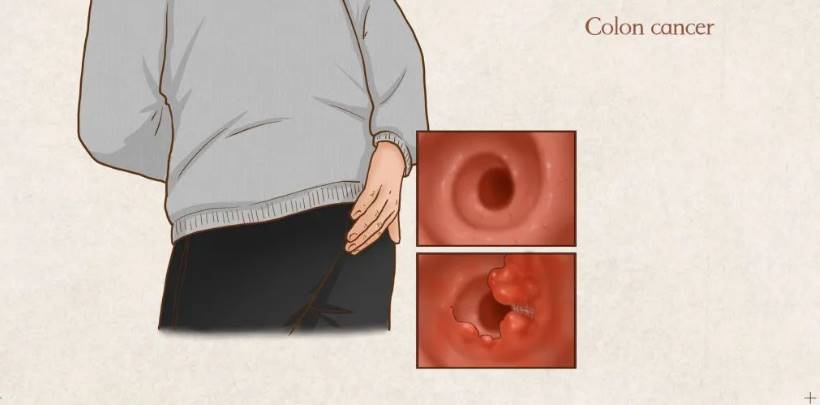
Colon cancer is commonly known as colorectal cancer. About 191,000 people die from this disease every year. Among those diagnosed, more than 70% are in the middle and late stages, and the 5-year overall survival rate is less than 40%. Usually, the earlier colon cancer is detected, the more likely it is to survive. It is possible to cure, so regular examinations, early detection, and early treatment are advocated. Colon cancer is also called the lucky cancer, mainly because the cure rate and 5-year survival rate are relatively high.
ADVERTISEMENT

Clinical treatment options for patients with colon cancerThe treatment of colon cancer is a long-term process. Abdominal radical resection of rectal cancer (Dixon) and abdominoperineal radical resection of rectal cancer (Miles) are two different methods of radical rectal cancer surgery. The main difference is whether to preserve the anus.
ADVERTISEMENT
Dixon surgery Suitable for rectal cancer in a high position, it refers to resection of the diseased rectum and anastomosis of the upper intestinal segment, sigmoid colon and lower intestinal residual segment, thereby retaining the function of the anus and allowing feces to be discharged normally through the anus; Miles surgery Resection of the diseased rectum, as well as the perineum, anus, and tissues around the anal canal, is generally done for tumors that are lower in position or have invaded the tissues around the anus.
The article is not finished. Click on the next page to continue.
ADVERTISEMENT
The article is not finished. Click on the next page to continue.
Next page
The Delco Road Rage Shooting Leaves 13 Bullet Holes in Car, Woman and Children Unharmed, Driver Charged with Attempted Murder
2024/08/15

Kylie Jenner Is a Must-See in Sexy ‘British Vogue’ Spread: See Her Dramatic Outfits
2024/08/15

Serial Killer on Death Row in California Admits to Cold Case Murder from 1986, Authorities Confirm
2024/08/15

6 New Country Tracks You Can’t Miss: Kelsea Ballerini, Scotty McCreery, and More
2024/08/15

A Delicious, No-Fuss Baked Chicken Thighs Recipe That’s Perfect for Busy Weeknights
2024/08/14

When Mike Miller Foulled Shaq and Only Hurt Himself: A Comical NBA Tale
2024/08/14

Julianne Hough Unveils the Genuine Reason Behind Her Split From Ryan Seacrest: ‘I’ve Come to Realize…’
2024/08/14

Beloved Actor Kyle Lowder Set to Reemerge as Rex Brady in ‘Days of Our Lives’
2024/08/14

Because the wife conceals the problem that she has no fertility, the man asks for divorce and does not divide the property, how does the view court judge?
2024/08/14

Essential Information as Taylor Swift’s Eras Tour Makes a Comeback in London
2024/08/14

‘It Ends With Us’: Blake Lively, Justin Baldoni, and the Cast’s Insights on Movie Production Amidst Feud Rumors
2024/08/14

Unlock Financial Freedom: How John Turned His Passion into a $5,000 Monthly Side Income in Just One Month
2024/08/14

Country Music Icon Jeannie Seely Recently Hospitalized in Pennsylvania
2024/08/14

From Debt to Dollars: A True Story of Financial Freedom
2024/08/14

Country Music Star Elle King Receives Backlash After Criticizing Her Father
2024/08/13

RHONJ’s Jackie Goldschneider on Letting Go of ‘Revenge’ Against Teresa Giudice
2024/08/13

La Grange Country Music Jam Makes an Enthusiastic Debut at Gordon Park
2024/08/13

Kit Harington Reflects on Game of Thrones’ Controversial Finale
2024/08/13

Hollywood’s Elite Embrace Salmon Sperm Facials: The Latest Anti-Aging Trend ?
2024/08/13

Hoda Kotb Reveals the Reason Behind Her Split with Fiancé Joel Schiffman
2024/08/13

